Popular
Tips for Controlling Blood
Pressure: What Diet & Exercise Can Do
Evelyn
Smith
MS
in Library Science, University of North Texas, 2012
Since
vascular dementia makes up ten percent of all dementia cases,
middle-aged and older adults should review these tips for helping to
control hypertension (Types of dementia, 2015, para. 5). Admittedly,
some of the tips for lowering the risk of Alzheimer's disease--such
as watching blood sugar by reading product labels, limiting carbohydrates and choosing
healthy fats, like olive oil and wild fish, cramming a minimum of 20
minutes of sustained aerobic exercise into a daily routine, and
lowering cholesterol levels—might also lower blood pressure (Rushlow, 2014, October 21, para. 78, & 10).
Although
concentrating on blood pressure might seem to take older adults back
to the days when dementia was synonymous with “hardening of the
arteries”, many of the tips for delaying or preventing Alzheimer's,
such as engaging in continuous aerobic exercise and keeping a
heart-healthy Mediterranean-style diet also substantially lower blood
pressure naturally. Anstey, Cherbuin, and Pushpani, for example,
identify eleven risk factors for Alzheimer's that include a high body mass
index (BMI) and a high serum cholesterol level, diabetes, smoking, and heavy
alcohol intake as well as four protective factors, such as
participating in high levels of physical activity and regularly
eating fish, that affect both cardiovascular health and the chance of
developing Alzheimer's or other types of dementia (Anstey, 2013,
August, Abstract).
References:
Anstey,
K. J., Cherbuin, N., Pushpani, M. H. (2013, August). Development
of a new method for assessing global risk of Alzheimer’s Disease
for use in population health approaches to prevention.
Accordingly,
anyone interested in delaying or preventing dementia should also look
into tips for lowering blood pressure, followed by longitudinal
studies that back up the recommendations as well as some occasional
helps to help readers achieve their heart and cardiovascular
system-healthy goals:
Maintain
a healthy weight;*
Be
physically active
[Exercise aerobically for at least 30 minutes at least five days per
week];*
Follow
a healthy
[DASH] eating
plan;*
Reduce
sodium in your diet;
Drink
alcohol only in moderation;
Take
prescribed drugs as directed.
(NHLBI,
2003, p. 17)
*Aerobic
Exercise & a Low Fat Diet Reduces Hypertension
 |
| Couple diet and exercise to reduce both your blood pressure and your waist line. |
So who needs to watch out for high blood pressure?
Hypertension risk
groups. (2014, March 30). Resperate. Retrieved
from http://www.resperate.com/hypertension/hypertension-risk-groups?utm_source=RESPeRATE+USA&utm_campaign=a4306ea230-LP_News_recipe_US_2015_4_16&utm_medium=email&utm_term=0_ac3cc1206e-a4306ea230-297127657&ct=t(LP_News_recipe_US_2015_4_16)
The overweight
(or those with a BMI over 25) as well as women and those in lower
income groups are most likely to have high blood pressure. Moreover,
according to a World Health Organization study, high blood pressure
is responsible for 12.5 percent of all deaths worldwide
(Hypertension, 2014, March 30, para. 1-2).
Risk
factors for high blood pressure:
- Obesity;
- Low income;
- Female
gender: High-income older women are more likely to try to actively
control their blood pressure;
- Heavy
drinking
(Hypertension,
2014, March 30, para. 3-4)
People from
all walks of life in hypertension risk groups
Even more those
who know they suffer from hypertension, the death rate for high blood
pressure is “strikingly high” in low and middle-income countries.
The WHO study also underlines the necessity of monitoring blood
pressure after age 40 since hypertension is a silent killer
(Hypertension, 2014, March 30, para. 5).
Hypertension
risk groups for secondary hypertension
Underlying
conditions—like Cushing's, Lupus, type 2 diabetes, and kidney
disease as well as taking oral contraceptives—can cause secondary
high blood pressure. Cocaine and amphetamines also raise blood
pressure (Hypertension, 2014, March 30, para. 6).
Accordingly, along with regularly monitoring for hypertension, adhering to a Mediterranean style diet along with fitting at least 30 minutes of aerobic exercise into a daily schedule, and loosing weight, so the Body Mass Index falls below 25, goes a long way toward controlling high blood pressure:
------------
Asikainen, T. M., Kukkonen-Harjula, K., and Miilunpalo, S. (2004). Exercise for health for early postmenopausal women: A systematic review of randomised controlled trials, 34(11), 753-78. Sports Medicine (Auckland, New Zealand). [Abstract only]. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/15456348
A systematic review of randomized, controlled exercise trials of post menopausal women aged 50 to 65 years reveals that early postmenopausal women can benefit from 30 minutes of moderate walking daily combined with a resistance training program twice a week, thus improving their flexibility, balance and coordination and decreases hypertension as well as lowering the abnormal amount of cholesterol and fat in the blood.
Bacon,
S. L., Sherwood, A., and Hinderliter, A. (2004). Effects of exercise,
diet and weight loss on high blood pressure. Sports
Medicine
(Auckland, New Zealand), 34(5), 307-16. [Abstract only]. Retrieved
from http://www.ncbi.nlm.nih.gov/pubmed/15107009
Exercise
alone reduces systolic and diastolic blood pressure approximately
3.5 and 2.0 mm Hg respectively.
Following
a DASH diet that emphasizes low-fat dairy products and fruits and
vegetables, reduces SBP and DBP 5.0 and 3.0 mm Hg respectively when
compared with following a standard American diet.
Both
exercise and weight loss decrease left ventricular mass and wall
thickness, reducing arterial stiffness and improving the functioning
of the inner lining of the blood vessels.
The
original DASH diet require the dieter to reduce his or her sodium
intake or lose weight to be effective, but recent findings show that
combining the original DASH diet with sodium reduction more
effectively lowers blood pressure than following the original DASH
diet plan alone. The DASH diet emphasizes fruits, vegetables, and
low-fat dairy products.
Glassberg,
H. and Balady, G. L. (1999,September-October). Exercise and heart
disease in women: Why, how, and how much? Cardiology
in Review,
(5) 301-8. [Abstract only]. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/11208241
One
quarter of all American adults are sedentary, and 1/3 of all women
don't take part in any leisure time physical activity. Studies,
however, note that women who exercise reduce their blood pressure and
improve their lipid profiles while lowering their likelihood of
developing diabetes. The Centers for Disease Control, the American
Heart Association, and the American College of Sports Medicine thus
recommend that everyone should participate in weight-bearing, aerobic
exercise at least three to five days per week. Aerobic exercise can
also help to prevent osteoporosis in women.
Hagberg,
J. M., Park, J. , and Brown, M. D. (2000, September). The role of
exercise training in the treatment of hypertension. Sports
Medicine
(Auckland, New Zealand), 30(3), 193-206. [Abstract only]. Retrieved
from http://www.ncbi.nlm.nih.gov/pubmed/10999423
Exercise
decreases blood pressure in approximately 75 percent of all
individuals diagnosed with hypertension. Women are more likely to
reduce blood pressure through exercise than men, and the middle aged
accrue more benefits from exercise than young adults and the elderly.
Low to moderate exercise also more efficiently reduced blood
pressure than high intensity exercise, and the more one exercises,
the greater his or her healthy benefits will be. However, a single
exercise session can reduce blood pressure for a 24-hour period.
Ishikawa-Takota, K.Ohta,T,
and Tanaka, H. (2003, August). How much exercise is required to
reduce blood pressure is essential to reduce blood pressure in
essential hypertensives? A dose-response study. American
Journal of Hypertension,
16 (8), 629-33. [Abstract only]. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/12878367
Previously
sedentary individuals diagnosed with hypertension can significantly
decrease their blood pressure by modestly increasing their physical
activity, according to the results of an eight-week exercise program
of 207 untreated subjects diagnosed with stage one or two
hypertension. Researchers divided participants into a control group
whose members exercised only 30 to 60 minutes per week, volunteers
who exercised from 61 to 90 minutes a week, 3) participants who
exercised from 91 to 120 minutes per week, and 4) individuals who
exercised over 120 minutes per week. Systolic and diastolic blood
pressure at rest didn't change for the control group, but individuals
in all other groups experienced a significant reduction in systolic
and diastolic blood pressure.
Lakka,
T. A. and Bouchard, C. (2005). Physical activity, obesity and
cardiovascular diseases. Handbook
of
Experimental Pharmacology,
(170), 137-63. [Abstract only]. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/16596798
Regular
physical activity for 45 to 60 minutes daily prevents unhealthy
weight gain and obesity whereas sedentary behaviors . . . promote
them.” The “optimal approach”, however, in weight production
programs combines regular physical exercise and a restriction of
calories. A minimum of 60 minutes of moderately intense physical
exercise, however, may be needed to avoid or limit weight gain in the
formerly obese.
Lin,
P. H., Ackin, M., and Champagne, C., et
al.
(2003, April). Food group sources of nutrients in the dietary
patterns of the DASH-sodium trial. Journal
of the American Dietetic Association,
103(4),488-96. [Abstract only]. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/12669013
The
DASH dietary pattern recommends that dieters drastically cut their
intake of meat, but they should increase their servings of fruits and
vegetables. That means consuming four to five servings of fruits,
four to five servings of vegetables, two to three servings of low-fat
dairy products daily while limiting servings of beef, poultry or fish
to twice a day, making up for this with four to five servings of
legumes, nuts, and seeds weekly.
Lin,
P. H., Appel, L. J., and Funk, K. (2007, September ). The PREMIER
intervention helps participants follow the Dietary
Approaches to Stop Hypertension
dietary pattern and the current Dietary Reference Intakes
recommendations. Journal
of the American Dietetic Association
107 (9), 1541-57. [Abstract only]. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/17761231
This
18-month, randomized, controlled trial followed 810 participants aged
25 and older with a BMI between 18.5 and 45.0, who were not taking
anti-hypertension medications and had been diagnosed with
pre-hypertension or stage one hypertension (SBP 120 to 159 mmHG and
DBP 80 to 95 mm Hg). Both the intervention group controls and those
participants who followed the intervention protocols as well as the
DASH diet plan substantially reduced their total fat, saturated fat,
and sodium intake and ramped up their intake of fruits, vegetables,
and dairy products. However, only those individuals who followed the
established intervention plan plus the DASH diet plan significantly
increased their intake of DASH specific food groups, rich in
potassium fiber, calcium, and magnesium. Researchers thus concluded
that a greater emphasis on “nutrient dense” food with improve
future dietary interventions.
Mendes,
R., Sousa, N., and Garrido,N., et
al.
(2014, November 12). Can a single session of a community-based group
exercise program combining step aerobics and body weight resistance
exercise acutely reduce blood pressure? Journal
of Human Kinetics,
43,49-56. doi: 10.2478/hukin-2014-0089. [Abstract only]. Retrieved
from
http://www.ncbi.nlm.nih.gov/pubmed/25713644
A
single, 50-minute session of exercise combining step aerobics and
body resistance training significantly reduced post exercise blood
pressure in a group of 23 healthy young women in their 30s. The
program consisted of a five minute warm up of aerobic dance
exercise, 30 minutes of step aerobics, 10 minutes of resistance
exercise training, and a five-minute cool down of breathing and
flexibility exercises.
When
an obese individual's BMI is greater than or equal to 30 km/m2,
mortality rates from all causes, especially cardiovascular disease,
increases by 50 to 100 percent. Thus, strong evidence exists that
weight loss in the over weight improves risk factors for diabetes and
cardiovascular disease. Weight loss reduces blood pressure in
overweight hypertensive and nonhypertensive [or prehypertensive]
patients, reduces serum TG levels, increases high-density lipoprotein
cholesterol levels, and may reduce low-density lipoprotein
cholesterol concentrates . . . Therefore, “30 to 45 minutes of
physical activity of moderate intensity should be encouraged. All
adults should set a long-term goal to accumulate at least 30 minutes
of moderate-intensity exercise on most, and preferably all days . .
.” Finally, those trying to lose weight after consulting a
physician should set a realistic weight loss goal of approximately
0.5 to one pound per week.
Schwartz,
J.B. (2015,April). Primary prevention: Do the elderly require a
different approach? Trends
in
Cardiovascular Medicine,
25(3), 228-239. [Abstract only]. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/25560975
While
trial data remains sparse for adults aged 75 to 80, primary
prevention strategy decisions at this stage of life should consider
estimated life expectancy and over all function as well as examine
cardiovascular event risks and access a benefit to harm ratio. Even
so, limited data supports the use of moderate aerobic exercise to
lower systolic hypertension, thus reducing the risk of cardiovascular
disease and dementia while also taking into consideration the
possibility that participants might fall and injury themselves while
exercising. While trial data on exercise alone is not available, a
review of “multi-system benefits” proves that exercise should
continue to be part of a preventive regime in the eldest elderly.
Solfriezzi,
V., Panza, F., and Frisandi, V. (2011, May). Diet and Alzheimer's
disease risk factors of prevention: The current evidence. Expert
Review of Neurotherapeutics,
11(5):677-708.
doi: 10.1586/ern.11.56. [Abstract only]. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/21539488
Elevated
saturated fats may help increase the effects of age-related cognitive
decline while current evidence links regular fish consumption
[usually amounting to at least two servings of fish rich in omega 3
fatty acids weekly] reduces the risk of dementia as does light to
moderate alcohol consumption [That amounts to a glass of red wine
with the evening meal]. Poorer cognitive function and an increased
risk of vascular dementia correlates with a low consumption of dairy
products, although research also links the consumption of whole fat
dairy products with cognitive decline. Adherence to a Mediterranean
diet slows cognitive decline as the elderly progress from Mild
Cognitive Impairment to full-blown Alzheimer's. Hence findings
encourage eating more fish, non-starchy vegetables and fruits in a
diet low in foods with added sugar.
____________
Skim
milk:
The calcium and Vitamin D in skim milk can lower blood pressure
from three to ten percent (Bauer, 2014, p. 1).
Spinach:
The potassium, folate, and magnesium in spinach can help lower
blood pressure (Bauer, 2014, p. 2).
Sunflower
seeds:
Unsalted sunflower seeds are “a great source of potassium”
Bauer, 2014, p. 3).
Beans:
The soluble fiber, magnesium, and potassium found in black, white,
navy, lima, pinto, and kidney beans lowers blood pressure and
improves cardiovascular health (Bauer, 2014, p. 4).
Baked
white potatoes:
Potatoes contain both magnesium and potassium. When a body's
potassium levels are low, it contains too much salt (Bauer, 2014, p.
5).
Bananas:
Bananas are “packed with potassium” (Bauer, 2014, p. 6).
Soybeans:
Soybeans contain potassium and magnesium (Bauer, 2014, p. 7).
Dark
chocolate:
Eating just 30 calories or a single square of dark chocolate daily
lowers blood pressures without gaining weight after 18 weeks
(Bauer,2014, p. 8).
DASH
[Dietary Approaches to Stop Hypertension diet] towards
lower blood pressure:
Emphasize
fruit, vegetables, and low-fat dairy selections;
Cut
back on saturated fat, cholesterol rich, and trans foods;
Consume
more whole grains, fish, poultry, and nuts;
Limit
sodium, sweets, sugary drinks, and red meats.
Reduce
salt intake:*
Don't
automatically reach for the salt;
Read
labels when shopping;
Select
fewer processed and packaged foods;
Ask
restaurant chefs not to add salt to menu selections, or choose
lower sodium options on restaurant menus.
Realize
that drinking moderately to lower blood pressure depends on other
lifestyle factors.
Develop
a sensible weight-loss plan:
Set
weight loss goals after deciding whether to participate in a
structured program or to simply limit portion sizes;
Understand
weight loss personalities: Impulsive, oblivious, uptight,
tenacious, or sociable;
Double-up
on diet and exercise: Only a combination of diet and exercise
leads to weight loss.
Adopt
a safe exercise plan:
Moderate
aerobic exercise for at lest 30 minutes daily at least five days
per week confers blood pressure lowering benefits.
To
stick with an exercise regime, “make it fun” and if possible,
“exercise with a friend”.
*Decreasing
Salt Intake
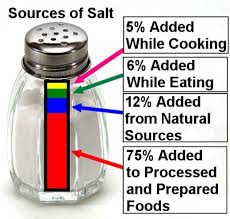 |
| Most salt comes from processed foods. |
He,
F. J., Li, J., and MacGregor, G. A. (2013, April). Effect of
long-term modest salt reduction on blood pressure. The
Cochrane Database of Systematic Reviews,
4, CD004937. doi: 10.1002/146551858.CD004937.pub2. [Abstract only].
Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/23633321
This
meta-analysis searched Medline, Embase, the Cochrane Hypertension
Group Specialized Register, the Cochrane Central Register of
Controlled Trials, and a reference list of relevant articles for
randomized trials that focused on a “modest” reduction of salt
intake and a duration of at least four weeks and found that a modest
reduction in salt intake for at least a month's reduction causes a
significant drop on blood pressure in hypertensive participants as
well as those with normal blood pressure irrespective of their gender
and ethnicity.
Rebholz,
C. M., Gu, D., & Chen, J., et
al.
(2012, October 1). Physical activity reduces salt sensitivity of
blood pressure: The Genetic Epidemiology Network of Salt Sensitivity
Study. American
Journal of Epidemiology,
Suppl. 7, S106-13. doi: 10 1093/aje/kws266. [Abstract only].
Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/23035134
A
dietary study conducted between October 2003 and July 2005 that
included a seven-day low-sodium intervention followed by a seven-day
high sodium intervention adhered to by 1,906 rural northern Chinese
age 16 and over found that physical activity may be “particularly
effective” in lowering blood pressure” among those individuals
who are “salt sensitive”.
Try
seasoning potatoes with pepper, parsley, onion, green peppers,
chives, or pimento (Seasoning without salt, 2015, para. 2).
Yang,
Q., Liu,T.,and Kuklina, E.V., et
al.
(2011, July 11). Sodium and potassium intake and mortality among US
adults: Prospective data from the Third
National Health and Nutrition Examination Survey.
Archives
of Internal Medicine,
171*13), 1183-91 doi: 10.1001/archintermed.2011.257. [Abstract
only]. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/21747015
The
Third National Health and Nutrition Examination Survey Linked
Mortality File (1998-2006), a prospective cohort study of a
nationally representative sample of 12,267 American adults
associated higher sodium intake with all causes of mortality.
Conversely, it also associated lower mortality risk with higher
potassium intake. Moreover, the individual's sex, ethnicity, BMI,
hypertension status, education and physical activity levels didn't
really differ. Accordingly, the findings suggest that a higher
sodium to potassium ratio correlates with an increased risk of
cardiovascular disease and all-cause mortality while a higher sodium
intake corresponds with an increased mortality rate in the general
United States population.
Zhang,
Z., Cogswell, M. E., and Gillespie, C., et
al.
(2013, October 10). Association between usual sodium and potassium
intake and blood pressure and hypertension among U. S. adults: NHANES
2005-2010.
PloS One,
10, 8(10), e75209. doi: 10.1371/journal/pone.0075289. [Abstract
only]. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/24130700
After
analyzing data on 10,563 study participants over age 20, who were
neither taking medication to control their blood pressure, nor were
on a low-salt diet, the National Health & Nutrition Examination
Survey found that the average intake of sodium, potassium, and
sodium-to-potassium ratios were 3,569 mhld, 2,745 mgld, and 1.41 mgld
respectively, so researchers thus concluded that the nigh sodium and
low potassium consumption levels correlated with hypertension.
A
Complete Physical Activity Program:
Include
aerobic and strength training activities in an exercise program, but
not necessarily in the same session, thus maintaining or improving
cardiovascular, respiratory and muscular fitness (Hagberg, 2011, p.
1, para. 1). The ACSM recommends 30 minutes of moderately intense
physical activity five days a week or 20 minutes of vigorous activity
three days a week to maintain cardiovascularhealth (Hagberg, 2011, p.
1, para. 2).
Aerobic
exercise includes walking, running, stair climbing, cycling, rowing,
cross-country skiing, and swimming (Hagberg, 2011, p. 1, para. 3).
Strength training should be performed at least twice weekly,
performing 8 to 12 reps of eight to ten different exercises that
target all muscle groups (Hagberg, 2011, p. 1, para. 4).
Treatment
Choices:
Once
under medications, individuals with hypertension can further
decrease their blood pressure through physical activity.
Mild
to moderate hypertension can also benefit from healthy lifestyle
changes, such as increasing physical activity, decreasing salt
intake improving diet, and losing weight.
Exercise
decreases systolic and diastolic blood pressure levels from five to
seven points as early as from three to four weeks after starting an
exercise program.
Physical
activity also helps control weight and improve blood pressure,
cholesterol, and glucose levels.
Individuals
diagnosed with ”pre-hypertension” (120 to 139 systolic pressure
and 80 to 89 diastolic pressure also need to exercise regularly.
(Hagberg,
2011, p. 1, para. 6)
How
Should You Exercise?
Beneficial
exercises include brisk walking, taking the stairs, moderate to
vigorous yard or house work, jogging, swimming, and cycling.
Moderate exercise may reduce blood pressure as much as strenuous
activity. The side affects of exercise, however, are “generally
positive” (Hagberg, 2011, p. 2, para.1-4).
Ways
to Improve Your Health:
Physical
activity can be added without making major lifestyle changes
(Hagberg, 2011, p. 2, para.5). Simple changes include parking
further away from destinations, taking the stairs, going for a walk
on the lunch hour, walking to a restaurant for lunch, taking children
to the park, mall walking in bad weather, waking up 30 minutes early
to exercise, and varying physical activities to make exercise
interesting (Hagberg, 2011, p. 2, para. 6).
Staying
Active Pays Off:
Moderate
physical activity significantly contributes to longevity, but
exercise can also help dieters stay on a diet and lose weight
(Harberg, 2011, p. 2, para. 7-8).
The
First Step:
Ask
some important questions that will access cardiovascular health
before increasing physical activity (Harberg, 2011, p. 2, para. 9).
Lifestyle
changes can lower blood pressure, possibly eliminating the need for
prescription drugs. Everyone, however, who suffers from high blood
pressure should look for natural ways to lower high blood pressure
(Harding, 2015, p. 1).
Exercise
more:
By exercising aerobically 30 minutes daily most days per week,
systolic blood pressure (the top number) can be lowered three to
five points, and diastolic blood pressure (the bottom number) can be
lowered two to three points. Pick an enjoyable activity and stick
with it (Harding, 2015, p. 2). Thus, everyone—whether one suffers
from hypertension or not—should take part in brisk aerobic
exercise for at least 30 minutes at a time five or six days per
week;
Eat
bananas
[or other foods high in potassium]: Select from choices like baked
potatoes with their skins, orange juice and non-fat yoga (Harding,
2015, p. 3);
Cut
salt:
Individuals already diagnosed with hypertension should limit their
salt intake to 1,500 milligrams daily, sticking with whole foods and
checking nutritional labels for sodium content (Harding, 2015, p.
4);
Don't
smoke:
Smokers average a higher risk for hypertension because lifestyle
factors often associated with smoking; for example, heavy alcohol
consumption and lack of exercise, increase blood pressure (Harding,
2015, p. 5);
Lose
weight:
Since extra weight makes the heart work harder, losing weight
lightens its cardiovascular work load (Harding, 2015, p. 6);
Cut
back on alcohol:
Drinking too much can elevate blood pressure. Accordingly, excess
drinking in both men and women increases the risk of hypertension
(Harding, 2015, p. 7);
De-stress:
Look for ways to manage stress (Harding, 2015, p. 8);
Yoga:
Yoga instruction teaches measured breathing that reduces
hypertension, which reduces hypertension since it modifies the
autonomic nervous system (Harding, 2015, p. 9);*
Skip
caffeine:
The caffeine in coffee, and to a lesser extent the caffeine in tea
and soda, causes short spikes in hypertension, so those diagnosed
with hypertension should limit their intake to two or less servings
of caffeine daily (Harding, 2015, p. 10); *
Meditate:
Daily meditation, whether it features chanting, breathing, or
visualization, lowers blood pressure (Harding, 2015, p. 11).*
*Yoga
& Meditation
 |
| Yoga and meditation reduce stress, lowering blood pressure. |
Bai, Z.,
Chang, J. & Chen, C.,
et al.
(2015, February 12). Investigating the effect of transcendental
meditation on blood pressure: A systematic review and meta-analysis.
Journal
of Human
Hypertension.
doi: 1038/jhh.2015.6. [Abstract only]. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/25673114
After
searching Medline, Embase, Cochrane Library, Web of Science, and
Chinese bio-medical literature databases for articles on
Transcendental Meditation through 2014, researchers first used the
Cochrane Collaboration's quality assessment tool, researchers zeroed
in on 12 studies that compared with TM groups with control groups.
They then discovered that TM had a greater effect on systolic blood
pressure among older participants, those with a higher initial blood
pressure rate, and women. As for controlling diastolic blood
pressure, TM works only as a short-term interventions for those
individuals already diagnosed with higher blood pressure.
Chu,
P., Gotink, R. A., and Yeh, G. Y. , et
al.
(2014, December 15). The effectiveness of yoga in modifying risk
factors for cardiovascular disease and metabolic syndrome: A
systematic review and meta-analysis of randomized controlled trials.
European
Journal of Preventive Cardiology,
pii: 204787314562741. [Abstract only]. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/25510863
After
reviewing 1,401 electronic records written in English found via
Medline,
EMBase,
CINAHL, PsycINFO, and the Cochrane
Central Register of Controlled Trials,
researchers found that compared to non-exercise controls, yoga
significantly improved body mass index, systolic blood pressure,
low-density lipoprotein cholesterol, and high-density lipoprotein
cholesterol. Significant changes also took place in body weight,
diastolic blood pressure, total cholesterol, triglycerides, and heart
rate. However, no significant differences existed between yoga and
exercise in their ability to bring down blood pressure.
Mashyal,
P., Bhargav, H., & Raghuran, N. (2014, October-December). Safety
and usefulness of Laghu shankha prakshalana in patients with
essential hypertension: A self-controlled clinical study.
Journal of Ayurveda and Integrative Medicine,
594), 227-35. doi:10.4108/9759475.131724. [Abstract only]. Retrieved
from
http://www.ncbi.nlm.nih.gov/pubmed/25624697
This
Bengalurui, India, self-controlled study recruited 32 patients
diagnosed with mild to moderate hypertension to participate in a
residential yoga therapy program. Patients took part in a daily
routine that featured six hours of yoga therapy that included
physical poses, relaxation sessions, pranayana and meditation as well
as the drinking of warm water. Participants significantly reduced
their systolic and diastolic blood pressure and pulse rates
immediately following yoga sessions. Moreover, after a week of yoga
therapy they also significant saw a drop in their blood pressure.
Eight
weeks of mindfulness meditation performed by those diagnosed with
pre-hypertension, but who as of yet weren't taking any medication,
didn't have any affect. However, researchers theorized that
meditation therapy might help patients already taking blood pressure
medications take them more consistently (Raven, 2013, October 4,
para. 2 & 5).
The
101 participants in the study averaged a blood pressure of 135/82 mm
Hg, above normal, but not yet “high”. Half started
mindfulness-based stress reduction (MBSR) immediately, but half were
wait listed to take the class later (Raven, 2013, October 4, para.
9-10). Mindfulness participants, aged 20 to 75, attended eight
weekly sessions as well as a day-long retreat and received
instructions to practice stress reduction therapy for 45 minutes
daily. Additionally, they received counseling that amounted to
standard-issue medical advice: Use less salt, quit smoking, and
exercise more (Raven, 2013, October 4, para. 11-12). A 2007 study
published by the US Agency for Healthcare Research Quality found that
Zen Buddhist meditation and Qi Gong “significantly reduced” blood
pressure (Raven, 2013, October 4, para. 17).
Telles,
S., Sharma, S. K., and Balkrishna, A. (2014, November 19). Blood
pressure and heart rate variability during yoga-based alternate
nostril breathing practice and breath awareness. Medical
Science
Monitor Basic Research, 20,
184-93. doi: 10.12659/MSMBR.892963.
[Abstract only]. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/25408140
Researchers
evaluated heart-rate variability, non-invasive arterial blood
pressure, and respiration rate during Alternate Nostril Yoga
Breathing (ANYB) and breath awareness sessions of 26 male volunteers
with the mean age of 23.8 years, assessing their performance five
minutes before the 25 minute yoga routines began, 15 minutes into the
exercise, and five minutes afterward, and they found that during
ANYB, the participants experienced a significant decrease in
systolic blood pressure as well as their respiration rate.
*Increasing
Potassium Intake
 |
| Bananas aren't the only foods rich in potassium. |
Miller,
Brian. (2015). 15 foods that are high in potassium. User's
Manual: Your Heart Health.
Health.com.
Retrieved from
http://www.health.com/health/gallery/0,,20721159,00.html
Decreasing
salt in taking and adding potassium-rich foods to a diet may cut the
risk of stroke by 21 percent. Since potassium protects blood vessels
from oxidation damage and keeps the walls of blood vessels from
thickening. While taking too much potassium as a supplement can be
dangerous, a potassium enhanced heart-healthy diet can provide the
4,700 milligrams of potassium adults need each day (Miller, 2015. p.
1).
The
following foods are rich in potassium: sweet potatoes, tomato sauces,
beet greens, beans, yogurt, clams, prunes, carrot juice, molasses,
cod, halibut, tuna, and rainbow trout,soybeans, winter squash,
bananas, milk, and orange juice (Miller, 2015, p. 2-16).
Potassium
triggers the heart to squeeze blood through the body, additionally
enabling muscle movement and nerve function as well as helping the
kidneys to carry blood (Potassium and your heart, 2014, para. 1-2).
Fruits and vegetables are the best sources of potassium, although
potassium is also found in dairy products, whole grains,meat, and
fish (Potassium and your heart, 2014, para. 3). A diet rich in
potassium lowers systolic blood pressure by ten points while taking
potassium supplements only lowers SBP lowers it by just eight points.
Many diets that lower cholesterol levels also are high in potassium
(Potassium and your heart, 2014, para. 6-7). The US Department of
Agriculture recommends that healthy individuals consume 4,700
milligrams of potassium daily (Potassium and your heart, 2014, para.
9).
A
2010 advisory committee found a short fall in United States potassium
consumption while moderate evidence associated potassium intake with
lower blood pressure. Adequate potassium levels also mitigate
age-related bone loss and the reduces kidney stones. Americans thus
need to increase their potassium intake above current levels for
optional health, although the affect of increased fruit and vegetable
consumption for short periods of time has proved disappointing.
Simultaneously, western diets have led to a decrease in potassium
intake with the reduced consumption of fruits and vegetables.
Consuming white vegetables, like potatoes, however, correlates with a
decrease in the risk of stroke. Potatoes remain the highest source
of dietary potassium provided the diner limits salt intake.*
Moreover, a low-potassium to sodium ratio strongly correlates with
cardiovascular risk.
Potassium
helps to lower blood pressure by “balancing out the negative
effects of salt”. Salt conversely reduces the kidneys' ability to
remove excess fluid. It's best to get potassium from natural sources
and avoid supplements (Why potassium, 2008, p. 1). Five servings of
fruits and vegetables daily should provide enough potassium to lower
blood pressure while also cutting the risk of certain cancers, bowel
problems, heart attacks, and stroke. Potatoes, sweet potatoes,
bananas, tomato sauce without the added salt and sugar, orange juice,
tuna, yogurt, and fat-free milk all are sources of potassium (Why
potassium, 2008, p. 2).
___________
If
I have high blood pressure, what can I do take care of myself?
Those
diagnosed with high blood pressure [as well as prehypertension] can
control their blood pressure in eight ways:
Eat
a better diet, which may include reducing salt;
Enjoy
regular physical activity;
Maintain
a healthy weight;
Manage
stress;
Avoid
tobacco smoke;
Comply
with medication prescriptions;
If
you drink, limit alcohol;
Understand
hot tub safety.*
(Prevention
& treatment of HBP, 2014, August 4, para. 1)
Lifestyle
modifications are essential since by adopting a heart-healthy
lifestyle, those at risk can
reduce
high blood pressure
prevent
or delay its development;
enhance
the effectiveness of blood pressure medications;
lower
the risk of heart attack, heart disease, stroke, and kidney disease.
(Prevention
& treatment of HBP, 2014, August 4, para. 2-4)
Here's
how to do your part:
Be
informed;
Do
your part to reach your treatment goals;
Change
your life and reduce your risks;
Take
medication if it is prescribed for you [if blood pressure is 140/90
or higher].
(Prevention
& treatment of HBP, 2014, para. 5-9)
Once
a treatment program becomes routine, maintaining a lower blood
pressure is easier (Prevention & treatment of HBP, 2014, para.
10).
Managing
blood pressure is a lifetime commitment, so take a pledge to do so
(Prevention & treatment of HBP, 2014, para. 11).
*Practicing
Hot Tub Safety
 |
| Those with high blood pressure should limit hot tub use. |
Individuals
with high blood pressure “should tolerate” saunas and hot tubs if
they aren't having a hypertensive crisis (Hot tub & sauna use,
2014, August 14, para. 1). Heat from these sources opens up blood
vessels in a process known as vasodilation that also happens after
taking part in brisk aerobic exercise (Hot tub & sauna use, 2014,
August 14, para. 2). Those diagnosed with high blood pressure
shouldn't move back and forth between cold water and a hot tub or
sauna since this could increase blood pressure. They also shouldn't
drink alcohol while using a sauna or hot tub (Hot tub & sauna
use, 2014, August 14, para. 3).
Sudden
or extended immersion in hot water can superheat the body and stress
the heart (Hot tubs, 2014, July 3, para. 1). Accordingly, if older
and middle-aged adults with potential cardiovascular problems receive
the go ahead to soak in a hot tub, they must regulate water
temperature, limit soaking time to no more than ten minutes, and stay
hydrated by drinking water (Hot tubs, 2014, July 3, para. 4).
When
the body super heats, blood vessels dilate to cool the body,
diverting blood away from the body core to the skin, so the heart
rate and pulse increase to counteract a drop in blood pressure (Hot
tubs, 2014, July 3, para.7). For those individuals with
cardiovascular disease, this could over tax the heart leading to a
loss of adequate blood pressure, a corresponding increase in blood
pressure, dizziness or faintness, nausea, abnormal heart rhythm,
inadequate blood flow to the heart or body, and heart attack (Hot
tubs, 2014, July 3, para. 5). Beta blockers and diuretics can further
contribute to the hot tub user's medical problems (Hot tubs, 2014,
July 3, para.6). Anyone using a Jacuzzi or hot tub should make sure
the water temperature isn't too high,should stay hydrated, and soak
for only brief periods of time (Hot tubs, 2014, July 3, para. 8).
Lose
extra pounds and watch your blood pressure:*
Men
are at risk if their waist measures more than 40 inches or 102
centimeters; Asian men are at risk if their waistline measures more
than 36 inches or 91 centimeters;
Women
are at risk if their waistline measure more than 35 inches or 91
centimeters—that's a Misses 16. Asian women are at risk if their
waistline measures more than 32 inches or 81 centimeters—that's a
Misses 10.
Exercise
regularly:
Eat
a healthy diet:
Reduce
sodium in your diet:
Europeans
and Asians under age 51 should limit sodium to 2,300 milligrams a
day or less; all African Americans and everyone over age 51 should
limit sodium intake to 1,500 milligrams daily.
Track
how much salt is in your diet: Record what you eat and drink.
Eat
fewer processed foods: Limit or eliminate potato chips, frozen
foods, bacon, and lunch meats.
Don't
add salt: Use herbs or spices instead.
Limit
the amount of alcohol you drink:
Avoid
tobacco products and second-hand smoke;
Cut
back on caffeine;
Reduce
your stress;
Monitor
your blood pressure at home and make regular doctor appointments:
Get
support from family and friends.
(10
Ways, 2012, July 19, p. 1-2)
*Weight
Management
 |
| Waist size predicts hypertension. |
Obesity
management interventions delivered in primary care for patients with
hypertension or cardiovascular disease: A review of clinical
effectiveness. (2014, July). Canadian
Agency for Drugs and Technologies in Health.
[Excerpt only]. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/25473691
Since
patients diagnosed with hypertension often fail to translate
behavioral changes associated with weight loss into long-term
behavioral maintenance, prescribing anti-obesity drugs might be a
good strategy for those patients that can safely tolerate this
strategy. Weight loss improves cardiovascular risk factors like
glycemic control and the reduction of cholesterol levels. Weight
loss, in turn, increases physical activity, reduces the risk of
atherosclerosis, cardiovascular events, stroke, and type 2 diabetes.
A reduction in triglycerides and an increase in HDL cholesterol
occurs with as little as a five to ten percent reduction in body
weight.
Tyson,
C.C., Appel, L. J., & Vollmer, W. M., et
al.
(2013, July). Impact of 5-year weight change on blood pressure:
Results from the Weight Loss Maintenance trial. Journal
of Clinical Hypertension.(Greenwich,
Conn.), 15(7), 458-64. doi: 10.1111.jch.12018. [Abstract only].
Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/23815533
Researchers
evaluated participants in a longitudinal weight loss maintenance
regime for weight loss, weight stability, and weight gain at a year,
30 months, and five years, respectively, observing correlations
between weight change and diastolic and systolic blood pressure.
Mean systolic blood pressure increased in participants who either
gained weight or maintained a stable weight, but they didn't increase
in the weigh loss group while diastolic blood pressures remained
stable for five years. These results thus suggest that continued
gradual, modest weight loss may sufficiently lower blood pressure in
the long term.
How
Abdominal Fat Increases Disease Risk
More
than sixty years ago a French physician associated larger waists
with a higher risk of premature cardiovascular disease (Vague, J.,
1947, La
diffrentiation sexuelle.
Facteur
determinant des formes de
l'obesity.
Press
Med.,
30, 339-40).
Since
then, follow-up studies have verified his finding while linking
abdominal-obesity with the risk of developing type 2 diabetes even
after controlling for Body Mass Index (BMI) (Waist size, 2015, para.
1).
Apple-
and Pear-shaped Body Types
Abdominal
obesity results in an apple-shaped body type. However, two popular
ways to determine abdominal obesity are measuring the waist's
circumference and determining waist size compared to hip-size, or the
waist-to-hip ratio (Waist size, 2015, para. 2-3).
Even
in those individuals who aren't otherwise overweight but who have a
large waist are at a higher risk for health problems than those with
a narrower waist. The Nurses' Health Study (2008),
which
looked at the relationship between waist size and deaths from heart
disease and cancer in middle-aged women, for example, found that
after 16 years women who had the largest waist sizes (35 inches or
higher) doubled their risk of heart disease when compared with those
women who had the smallest waist size (less than 28 inches).
Moreover risks increased with every added inch to the waist (Waist
size, 2015, para. 4-5). Even women was a normal BMI were at risk if
they carried more of their body weight around the waist (Waist size,
2015, para. 6). The Shanghai Women's Health Study (2007) came up
with the same findings (Waist size, 2015, para. 6).
Larger
waists are so risky because the fat surrounding the liver and other
abdominal organs is metabolically active, thus releasing fatty acids,
inflammation, and hormones that lead to higher LDL cholesterol,
triglycerides, blood glucose levels, and a rise in blood pressure
(Waist size, 2015, para. 7).
Which
Is Best: Waist or Waist-to-Hip?
A
2007 study associated both waist-to-hip and weight circumference with
cardiovascular risk while additional studies have found they predict
future type 2 diabetes, heart disease, and cancer diagnoses (Waist
size, 2015, para. 8-9).
__________
Go
for power walks:
Walk briskly for at least 30 minutes daily;
Breathe
deeply:
Practice qigong, yoga, or tai chi;
Pick
potatoes:
Regularly include potassium-rich foods, like potatoes, in a
heart-healthy diet;*
Be
salt smart:
Cut sodium by stirring away from processed foods;
Indulge
in dark chocolate
[in moderation];.
Take
a supplement:
Ask the family doctor about taking coenzymeQ10;
Drink
a little alcohol:
Moderate drinking lowers blood pressure;
Switch
to decaf coffee;
Take
up
[hibiscus] tea;
Work
a little less
[more than 41 hours per week];
Relax
to music:
Listen to soothing, classic, Celtic, or Indian music for 30 minutes
daily];*
Seek
help for snoring;
Jump
for soy
[as well as nuts].
Obviously,
all cooked foods need to be broiled, grilled, or boiled rather than
fried.
*Taking
up Hibiscus Tea:
 |
| Drinking hibiscus or tisane tea lowers blood pressure. |
Some
researchers think hibiscus might be an effective treatment for high
blood pressure. WebMD
reviews rate it “possibly effective” along with such common
alternative treatments for high blood pressure and hypertension as
co-enzyme Q-10, fish oil, and potassium while not enough evidence
exists to truly evaluate whether soy is an effective treatment for
high blood pressure.
Hopkins,
A. L., Lamm, M. G., and Funk, J. L. et
al.
(2013, March). Hibiscus sabdarrffa
L. in the treatment of hypertension & hyperlipidemia: A
comprehensive review of animal and human studies. Fitoterapia,
85 (84-94). doi: 10.2026/j.fitnote.2013.01.003. [Abstract only].
Retrieved from
Hibiscus
sabdarrffa is a home remedy for treating hypertension and
hyperlipidenia without adverse side effects unless less taken in
high doses, although it does act as a diuretic. Animal studies show
that Hibiscus sabdarrffa extract reduces blood pressure in a dose
dependent manner, and randomized clinical trails show that hibiscus
tea significantly lowers systolic and diastolic blood pressure in
adults with prehypertenson as well as moderate hypertension and type
2 diabetes, making it at least as effective at lowering blood
pressure at Captropril, but less efficient than
Lisinopril.
McKay,
D. L., Chen, C.Y., and Saltzman, E., et
al.
(2010 February). Hibiscus sabdariffa L. tea (tisane) lowers blood
pressure in pre-hypertensive and mildly hypertensive adults. The
Journal of Nutrition,
140(2), 298-303. [Abstract only]. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/20018807
A
randomized, double-blind placebo controlled six week trial of 65 pre-
and mild hypertensive adults age 30 to 70 not taking blood pressure
lowing medications found that daily drinking three 240 milliliter
servings of hibiscus
tea lowered systolic blood pressure when compared with a placebo. Tea
sippers with a high systolic blood pressure at baseline exhibited a
greater response to hibiscus tea.
*Relaxing
to Music:
 |
| Classical Indian music lowers blood pressure. |
Brookes,
Linda. (2005). Significantly new definitions, publications, risks,
benefits: Music can reduce blood pressure, depending on the tempo.
Medscape
Multispecialty.
Retrieved from http://www.medscape.org/viewarticle/514644_6
Listening
to music with a fast tempo increases blood pressure while listening
to slower music lowers it. Introducing a pause, in turn, lowers
blood pressure even further, and these effects particularly apply to
individuals who have had musical training, according to a study
published in the British medical journal, Heart (Brookes, 2005, para.
1). Study participants in Italy and the United Kingdom listened to
six selections played in random order whereupon researchers
documented that faster tempos and simpler rhythmic structures
increased ventilation, breathing rate, systolic and diastolic blood
pressure, mid-cerebral artery flow velocity and heart rate while
slow music exercised less effect, although Indian raga induced a
“significant drop” in heart rate (Brookes, 2005, para. 2-4).
*Jumping
for Soy:
 |
| Soy can lower blood pressure, but it does have its own hazards. |
Mohammadifard,
N. , Salehi-Abarghovei, A., and Salas-Salvado, J. (2015, March). The
effect of tree nut, peanut, and soy nut consumption on blood
pressure: A systematic review and meta-analysis of randomized
controlled clinical trials. The
American Journal of Clinical Nutrition.
pii. Ajcn091595. [Abstract only]. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/25809855
Scanning
Medline, SCORPUS, ISI Web of Science, and Google Scholar between 1958
and October 2013, researchers found that nut consumption leads to a
“significant reduction” in systolic blood pressure in study
participants without type-2 diabetes. Pistachios most effectively
reduced systolic and diastolic blood pressure.
Stradling,
C., Hamid, M., & Fisher, K., et
al.
(2013, December). A review of dietary influence on cardiovascular
health: Part 1. The role of dietary nutrients. Cardiovascular
& Hermatalogical
Disorders
Drug Targets,
13(3), 208-30. [Abstract only]. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/24304234
Upon
searching the Cochrane Library database between 2006 and 2012,
researchers found evidence that “underpins current dietary
cardiovascular guidelines—replacing saturated and unsaturated fat,
consuming whole grains or carbohydrates of low on the glycaemic
index, increasing the consumption of fruit, cruciferous vegetables,
nuts, and oily fish. Additionally, adding soya protein to one's diet
and reducing sodium intake reduces cardiovascular disease risk.
Furthermore, dietary changes, such as consuming fewer animal and
processed foods, results in a reduction in saturated fats.
____________
Selected Research Studies on the Affect
of Diet upon Blood Pressure

Research
also suggests that a diet that emphasizes fruits and vegetables as
well as including at least two servings of oily fish per week in the
diet help to lower blood pressure and improve cardiovascular health
and ward off Alzheimer's at the same time.
Afolayan,
A. J. & Wintola, O. A. (2014, April 3). Dietary supplements in
the management of hypertension and diabetes—a review. African
Journal of traditional, complementary, and alternative medicines:
AIRCAM/African Networks on Ethnomedicines,
11(3), 248-58. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/25371590
Orthodox
drugs used in the treatment of hypertension and diabetes may produce
adverse side affects like headaches, nausea, vomiting, stomach pain,
constipation, diarrhea, weakness, fatigue, and erectile dysfunction.
However, relying on vitamins, minerals, amino acids, herbs and other
botanical treatments as well as a diet that emphasizes fruits and
vegetables in many instances provide safer and less expensive
alternatives to conventional pharmaceuticals particularly in
third-world countries.
Mori,
T. A. (2014, September). Omega-3 fatty acids and cardiovascular
disease: Epidemiology and effects on cardiometabolic risk factors.
Food
& Function,
5(9) 2004-19. doi: 1039/c4fo009d. [Abstract only]. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/25062404
Clinical
and epidemiological studies support evidence that polyunsaturated
omega-3 fatty acid from fish and recommended dosages of fish oil
protects the cardiovascular system, favorably influencing risk
factors for blood pressure, vascular reactivity, and cardiac function
without being associated with any adverse effects, including the risk
of heavy bleeding. Health professions thus recommend two serving of
fish weekly. The general population should incorporate these
servings of fish in a diet plan that increases the consumption of
fruits and vegetables while moderating salt intake.
Rees,
K. Hartley, L., and Floers, N. et
al.
(2013, August). 'Mediterranean' dietary pattern for the prevention
of cardiovascular disease. The
Cochrane Database of Systematic Reviews,
12(80. CD009825. doi: 1002/14651858.CD009825.pub2. [Abstract only].
Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/23939686
After
the Seven Countries Study found in the 1960s that countries
surrounding the Mediterranean experienced lower cardiovascular
disease mortality rates than Northern Europe and North America,
observational studies confirmed these findings, but clinical evidence
documenting the diet's benefits for the most part was lacking until
researchers searched electronic databases from 1946 to 2012. A
Mediterranean diet by definition has a high monounsaturated to
saturated fat ratio and features low to moderate red wine intake as
well as a high consumption of legumes, grains, cereals, fruits, and
vegetables while severely limiting meat and meat products while
increasing the amount of fish eaten, and only consuming dairy
products in moderation. Researchers eventually included 11 trials
and 15 papers in their survey, and this limited evidence suggests
that following a Mediterranean diet may benefit cardiovascular
health.
Wanjek,
Christopher. (2015, March). 'MIND ' your diet and protect against
Alzheimer's. Yahoo.com. Retrieved from
http://news.yahoo.com/mind-diet-protect-against-alzheimers-144212880.html
Following
the MIND diet as documented in the Online March issue of Alzheimer's
and Dementia, results in a 35 percent reduction in the risk of
Alzheimer's (Wanjek, 2015, March 25, para. 2, 4, & 11). The MIND
diet, which combines the DASH and Mediterranean diets, emphasizes
green leafy vegetables, along with other vegetables, nuts, berries,
beans, whole grains, fish poultry, olive oil, and wine. Conversely,
MIND dieters should avoid red meat, butter and stick margarine,
cheese, pastries, and sweets (Wanjek, 2015, March 25, para. 10).
___________
Addendum
August
31, 2015
The American Heart Association recommends that healthy
adults eat two servings of Omega-3 fatty fish weekly, although the University
of Maryland Medical Center cautions that three servings of Omega-3 fish week
may raise the rise of hemorrhagic stroke.
The Website also cautions that it’s important to consult a physician
before taking more than three grams of Omega-3 fatty fish capsules daily (Omega
3 fatty acid, 2015, para. 8 & 21).
Omega 3 fatty acids. (2015). University of Maryland Medical Center. Retrieved from http://umm.edu/health/medical/altmed/supplement/omega3-fatty-acids
___________
The links furnished on this Web page represent the opinions of their authors, so they complement—not substitute—for a physician’s advice.


